
Food as Homework
What Food and Medicine and the new SNAP restrictions have in common

 : r/MovieQuotes")
Even if you haven’t seen Alex Garland's Civil War, you might be familiar - from memes like this - with a scene in which Jesse Plemons, in sunglasses, standing over captives by a mass grave, asks: "What kind of American are you?"
The answer determines whether you live or die. The person asking already knows which answers are acceptable, though the person answering is unsure whether ‘Missouri’ is a better answer than ‘Florida’.
It’s a scene that came to mind unbidden when I was reading about the recent restrictions on Supplemental Nutrition Assistance Payments (SNAP) in the US, and the chaos they’ve caused working families here.
In the name of public health, working class people who qualify for state support for food purchases have complex restrictions on what they are and aren’t allowed to buy. Candy and soda are verboten, but the definitions of what counts as candy and soda vary state by state. At a grocery checkout in Iowa, a granola bar is candy if it doesn't contain flour, but a Twix isn't candy because it does contain flour.
The question at the checkout is the same one Plemons is asking: not what food are you buying, but what kind of food buying are you doing? The SNAP benefit card in your hand — the one that may or may not work for the items in your cart — determines whether you’ve chosen wisely or will need to suffer the indignity of returning your purchases.
The checkout isn't the only place where working class families face this kind of sorting. It's been formalized into clinical research.
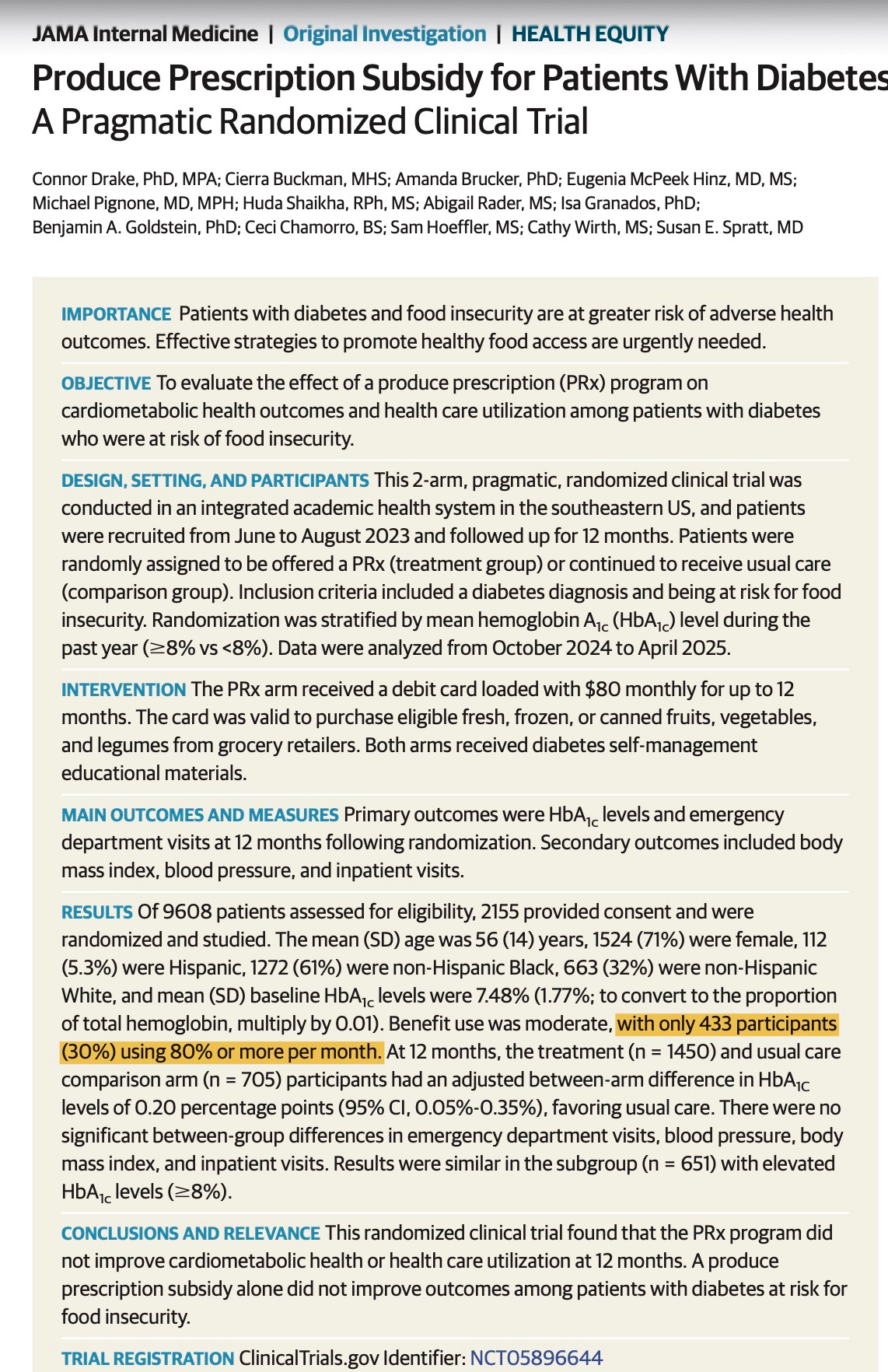
JAMA Internal Medicine recently published what I imagine, when the grants were applied for, was going to be the landmark study on Food as Medicine. It was set to answer, definitively, the question of whether doctors can prescribe food and make people healthier.
Over two thousand people with diabetes and at risk of food insecurity were recruited, and the experiment lasted over a year. In the trial, participants got an $80/month debit card that could only be used for certain kinds of food. Their blood A1c was monitored and, after a year, the finding was supposed —finally — to answer the question about whether prescribing food was a good way to reduce the effects of diabetes.
The answer: for patients at risk of food insecurity it’s a little bit worse to prescribe food in addition to providing usual care than merely to offer the current standard of care.
Look closer, and you’ll spot a problem.
The problem is that, for reasons undisclosed in the article, participants didn’t stick with using the restricted debit card:
433 participants (30%) used 80% or more of their subsidy on average for more than 10months, 197 (14%) used 60% to 79% of their subsidy for longer than 10 months, and 516 (36%) used their subsidy to a lesser degree than the previous 2 groups.
To put it differently, the largest group of people did use the debit card at least once, but decided not to after that. One possible reason is the debit card itself. Who knows whether, when you get the checkout, your debit card will work for the stuff in your cart?
If someone gave me a monthly $80 debit card for “eligible fruits, vegetables, and beans (fresh, frozen, or canned without added sugar, salt, and fats)”, they’d not be giving me food; they’d be giving me homework.
For folk holding down multiple jobs, with limited time and money to shop and scratch cook, processed food might be an important way to balance nutrition, income, and health. That’s not to say folk don’t want to eat healthier food. But dignity at the check-out matters, and no-one wants to have to return an ineligible purchase. Beneficiaries already feel shamed by having to split purchases into two batches, one for benefits and another without.
The states that have rushed to impose SNAP restrictions are overwhelmingly, though not entirely, Republican. The Food as Medicine movement comes from the other direction — from progressive public health researchers, from liberal foundations, from people who would be appalled by the cruelty of cutting a family’s benefits because they bought the wrong granola bar. But both begin from the same premise: that the problem with hungry people is the choices they make, and that the solution is to structure their choices for them.
This is a bipartisan consensus. Liberals and conservatives might disagree about whether the poor deserve punishment or treatment, but they do not disagree that the poor are making the wrong decisions about food.
New labelling initiatives for UPF-Free, or California Certified double down on these politics. They don't regulate what's manufactured; they add another checkpoint at the shelf, another moment where the consumer is sorted. If you're faced with local or organic or UPF-free or, better still, two out of three of these, what should you buy? And how much shame should you feel when you're standing in the aisle doing arithmetic that the food industry never has to do?
The food environment in which these choices happen — what's on the shelf, what it costs, how it got there, who engineered it to be cheap and shelf-stable and irresistible — is treated as given. The market that has made ultra-processed food the rational choice for anyone short on time and money is not subject to restriction, not up for clinical intervention, not being asked to present its card for inspection, not itself an acceptable task for homework.
You can regulate what a person on SNAP buys. You cannot, it seems, regulate what a corporation puts on the shelf. And you certainly cannot ask why the person is hungry in the first place.
"The notion that the food system can be transformed through individual acts of consumption—rather than through lobbying, organizing, boycotts, mobilization, or direct action—fits nicely within the prevailing neoliberal economic rhetoric: that unregulated capitalist markets yield the most efficient allocation of resources." (Eric Holt-Giménez and Yi Wang, 2011).
I appreciate your critique of both SNAP restrictions and "Food as Medicine" – conservative and liberal food policies – for continuing the same underlying narrative that emphasizes individual action rather than structural change. Dominant politics argue about the most efficient policies to address food insecurity without addressing the basic question of: WHY are people hungry to BEGIN with?
Thank you for writing this. I have been reading the multitude of Food is Medicine literature that has been produced recently and have felt the same. Its validating to hear similar thoughts from an expert. The studies and reports assume most people don't understand "food is medicine", that they don't know that nutritious food is good for them at the most basic level. Most of commentary centers the consumer and nitpicks her choices and suggests strategies to manipulate those tiny choices.
All of this in an environment where we allow the prices of eggs and dairy to fluctuate wildly like the stock market does while we have 19 different flavors of boxed mac and cheese in the center aisle at much more stable and affordable prices.